


An Elegant Solution for U.S. Health Care System Reform
How a universal primary care system could solve many ills in American health care

While surprisingly absent from the campaign trail in 2024, health care remains a key issue for Americans. Care is too expensive, insurance premiums continue to rise faster than wages, and practices like prior authorization are rampant.
The Patient Protection and Affordable Care Act (ACA) was the most recent attempt at redesigning the US health system to solve key problems and improve performance. Yet, it is clear that while parts of the ACA were steps in the right direction, it was not enough to solve major challenges and to help the US system perform on par with other countries.
The larger political debate usually centers around whether the US should adopt a universal health coverage system (e.g., Medicare-for-All) like our economic peer countries, or remain a hybrid, mostly private, mixed for-profit-non-profit system. The fact is that the US system has elements of both already, but therefore does not benefit fully from either the positive market shaping forces of competition in a true free-market system or the central regulation of a fully-government operated system.
I am a true believer in the value of competition and the free market, but, to be clear, we do not have this in the US.
To put it bluntly, the system sucks. Yet political narrative around the issue has falsely characterized the debate as one of socialism vs capitalism in a country that has deeply rooted anti-socialism political leanings. However, this is an issue that should not be politicized as there are clear system design components that lead to the better performance seen in our peer countries and that would offer much better health and quality of life for Americans.
But, this is not an article to argue for or against the predominant proposals. I already discussed some parts of that discussion in a previous article. This is about a more elegant, effective, and innovative policy solution: government-operated universal primary care.
Note: this is a descriptive article about a concept. It is not a comprehensive plan, analysis or roadmap.
The Current U.S. Healthcare Landscape
The American health care system relies primarily on employer-funded private health insurance (48.6% of population), Medicare for adults older than 65 (14.7%), and Medicaid (21.2%) for low-income families, children, pregnant people, and individuals with disabilities. Another 6.2 percent of the population is covered by non-group private plans, 1.3 percent of the population is covered by the military health system, and 7.9 percent are uninsured. Most working Americans receive health insurance through their employers, who typically share premium costs with employees. For those without employer coverage, options include purchasing individual plans through the Affordable Care Act marketplaces or qualifying for government programs. This primarily employer-based system emerged as an accident of history during World War II wage controls, when companies used health benefits to attract workers.
The fragmented nature of this system creates inherent inefficiencies. Insurance companies negotiate different rates with different providers, leading to variable pricing for identical services. Administrative costs multiply as health care providers must interact with numerous insurance companies, each with their own procedures and payment systems. Indeed, estimates suggest that administrative burden consumes about 1/6th of a physician’s working hours.
Not only is the system inefficient and burdensome, but it also performs worse than other countries. The US spends more on health care than any other country, but Americans get poorer quality and a lot of anger-inducing, administrative barriers.
Across the Atlantic, the United Kingdom took a radically different path. In the aftermath of World War II, while American companies were beginning to offer health insurance as a job benefit, Britain was creating the National Health Service (NHS). The NHS emerged from a vision that health care should be available to all, regardless of wealth. Today, if you walk into a primary care office in London, you won't see a billing department or insurance verification desk. Instead, you'll find a straightforward system where doctors focus on patient care rather than a complex web of insurance rules.
This is where the very hot debate about what to do about this problem begins. Americans hate their expensive health system, they hate insurance companies, and they generally hate the profiteering; so, many proponents suggest that since other countries perform better with universal health care coverage and careful price regulation we could solve these problems through a similar system.
But, free-market advocates argue that the problem lies in too little competition, suggesting that removing regulations and increasing price transparency would drive down costs while improving quality1. They point to examples like LASIK eye surgery, where market competition has indeed led to lower prices and improved technology. Universal health care proponents counter that health care isn't like other markets—when you're having a heart attack, you can't shop around for the best price on emergency cardiac care. Economists call this inelastic demand, where the demand for services remains relatively constant regardless of price. Price and quality are usually the two attributes by which consumers compare products, but in the US both are difficult for consumers to assess. I have a previous article on this topic here.
Where does all the money go?
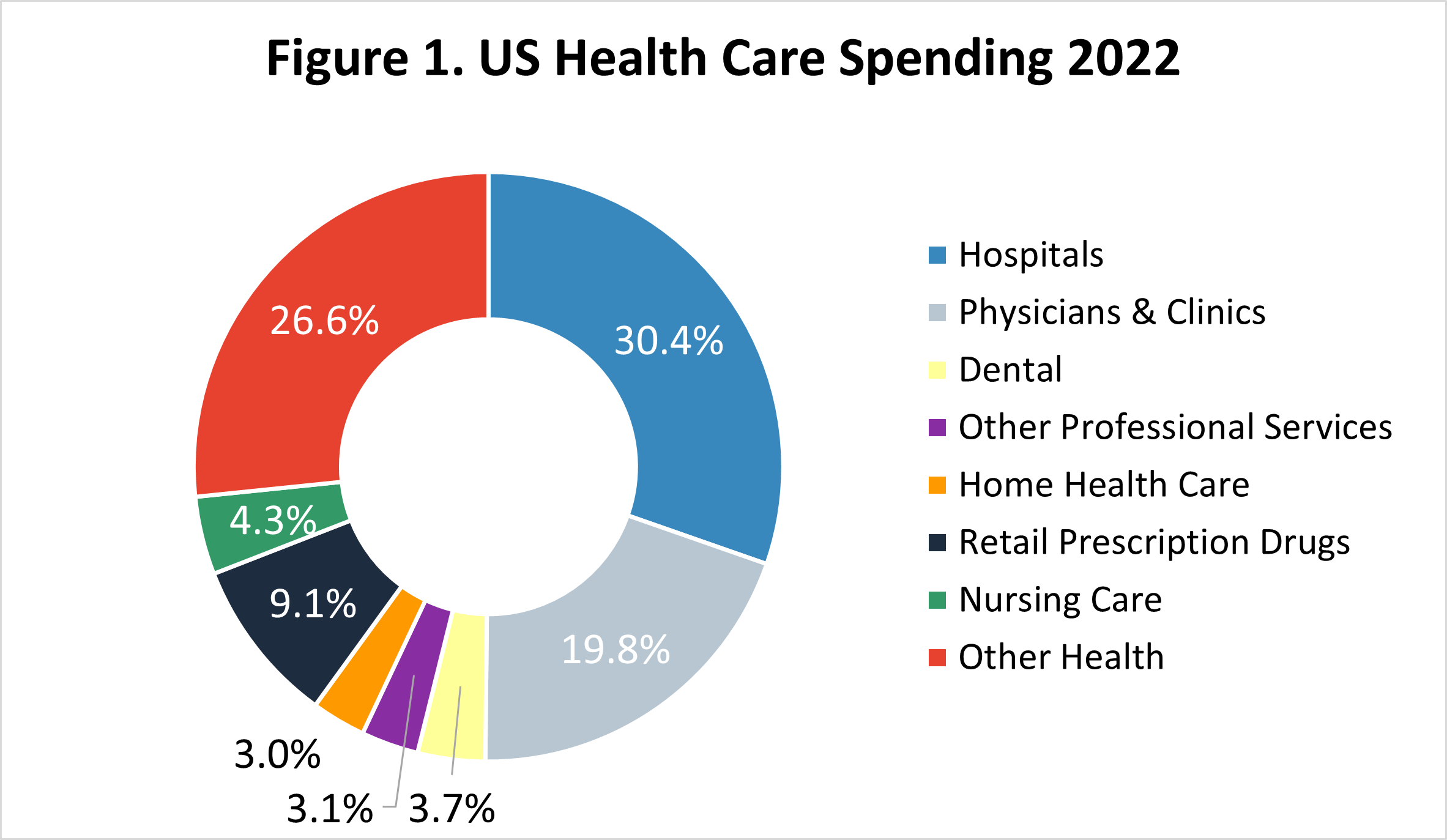
According to the Peterson-KFF Health System Tracker, the US spends the majority of its health care dollars on hospitals at 30.4% of the $4.5 trillion spent in 2022 (Figure 12). This is followed by “other health” which is comprised of durable medical equipment and non-durable products at 26.6%, physicians and clinics at 19.8%, and retail prescription drugs at 9.1%.
The US spent $12,197 per capita in 2021 vs an average of $6,514 in other economic peer countries. Specifically, the US spends over two times as much on hospitals & expensive outpatient care ($7,500 per capita compared to $2,969 in other countries), three times as much on administration, and almost 2 times as much on prescription drugs and medical goods.
The Role of Primary Care in Spending and Health
While the US spends ~19.8% on physicians and clinics, the majority is spent on expensive specialists and services that treat already advanced chronic conditions rather than on high-value, prevention-focused primary care. The US spends between 5.4% to 6.5% on primary care, historically. Estimates in 2019 suggest that number was 7% with lower amounts of spending for patients on Medicare (5.3%) and those in worse health (5.6%). The researchers estimate the average dollar amount is about $439 per person per year. Other economic peer countries spend about 13% (nearly double the US spending).
Primary care is critical because it is where critical prevention and health promotion activities occur. While medical care alone is not enough to improve the public’s health3, primary care access and spending represent a great opportunity to reduce total US spending on hospitals, specialists, and expensive medical devices.
Research comparing countries suggests that a larger national investment in primary care results in lower costs, higher patient satisfaction, and can reduce emergency care and hospital utilization4. It is clear that the lack of US investment in primary care services is a major contributor to poor performance.
Universal Healthcare Systems: The UK and Canadian Models
In contrast to the US, both the United Kingdom and Canada operate universal health care systems. The UK's National Health Service (NHS) represents a fully nationalized system where the government owns most hospitals and employs health care workers directly, funded through general taxation. The central government agency, NHS England, sets requirements and distributes funds to 191 local Commissioning Groups that organize and manage care at the local geographic level. All residents of the UK are enrolled and have access to this public system and most care does not require out-of-pocket spending at the point of care. Also, around ten percent of the population carries additional voluntary supplemental insurance to have faster access to care.
Family doctors, known as General Practitioners or GPs, serve as the system's foundation. Most GPs aren't government employees—they're independent contractors who run their own practices but work primarily for patients covered by the NHS, though they can take private paying clients as well. When a British citizen needs care, they visit the local GP of their choice, with whom they are registered and assigned, who can either treat them directly or refer them to an NHS-employed specialist at an NHS hospital. Payment from the NHS to GPs is negotiated by the British Medical Association where 60% of the payment is capitation, or a monthly payment per registered patient, 15% is fee-for-service, and 10% is linked to performance.
North of the U.S. border, Canada developed yet another approach to universal health care. Similar to Britain's more centralized NHS, Canada's Medicare system is a patchwork of provincial and territorial health insurance plans, bound together by federal standards. Walking into a doctor's office in Toronto feels more similar to an American experience than a British one—the facilities are typically private practices, and doctors run their own offices. The key difference? When it comes time to pay, there's only one insurance plan to bill: the provincial health authority. This significantly reduces administrative complexity and adverse profit motives present in the US system.
Comparative Performance: High Costs, Poor Outcomes
The contrast in outcomes between these systems is stark. Despite spending nearly twice as much per person on healthcare as either Britain or Canada, the United States lags behind on virtually every measure of health system performance (see Figure 2). American life expectancy is lower, infant mortality is higher, and preventable deaths occur more frequently. Perhaps most troubling, Americans regularly report avoiding necessary medical care due to cost—something virtually unheard of in other developed nations.
Figure 2: Commonwealth Fund Country Health System Overall Performance Ranking5

Lower life expectancy
Higher infant mortality rates
Higher rates of preventable deaths
Longer wait times for many procedures
Lower rates of primary care visits per capita
Focusing US Health System Redesign on Primary Care and Prevention
Imagine a system in which every American could visit a primary care doctor without worrying about payment, while maintaining the current private insurance system for specialty care and hospitalizations. What if we changed the narrative around universal health care and focused on the narrow services to be offered via a universal primary care system. Let’s call this system the US National Primary Care System (USNPCS) that could be administered by the US Center for National Primary Care, an agency of the US Department of Health and Human Services.
This system would carve out a defined set of benefits and services from all other insurance coverage systems and allocate it to the new agency. This agency would operate like a hybrid between the current Centers for Medicare and Medicaid Services and the Veterans Health Administration wherein most of the funding would be paid to medical practices owned and operated by primary care practitioners. But, some government-operated clinics would be launched in areas with limited access to care via a hub-and-spoke model that leverages telemedicine to reach rural and hard to reach areas in a cost-effective manner.
These programs would be managed via trusts at the US state-level to align the program with local needs, to allow for state fund allocation, and to maintain the federal-system spirit.
How much money do we need to do this?
Let’s first carve out the defined set of services that represent primary care services from the existing coverages using the $439 current spending per capita multiplied times the US population to get to ~$147 billion dollars. This should be budget neutral as a starting point.
Then, we need administrative costs for the agency and we want to increase the amount of investment in primary care from the current US levels to the OECD average of 13%. Thus, we want to invest $815 per American in primary care services, so that would require a total funding of $273 billion dollars or an incremental increase of $126 billion in spending.
To derive administration costs, we can use CMS as an analog. CMS spends about 1 - 2% of program costs on internal administration. Let us use 3% for our purposes as there are some start-up challenges and added expense in operating clinics in certain areas. This brings the total costs up to about $281 billion, of which $147 billion is budget neutral as it has been derived from other programs. Employers would pay in their share via a tax equivalent to the carve out, states would pay their share of Medicaid savings, and Medicare would contribute as well. That leaves $134 B to cover.
How to pay for the new agency?
There are two clear methods by which to pay for this system. First, one might argue that improved primary care will result in lower demand for hospital services, and specialists. The central system will also lower administrative burdens by allowing clinics to manage a single payor relationship. Thus, money could be reallocated from these areas to fund the USNPCS. For example the 30.2% hospital spend of the $4.5 trillion in total spending is $1.44 trillion. About $606 Billion of that is Medicare and Medicaid, so a 5% reduction in payments yields about $30.3 billion toward the USNPCS. It is reasonable to expect that universal access could yield a 5% or more reduction in spending, anything further would be a net savings. Using $63,000 as the average US salary, a payroll tax of 0.5%6 half funded by employers and half funded by employees would yield $106 billion. That would be an average tax of $157.5 per person per year or $13.1 per month.
This would cover the system. In the event that this system has the expected effects of reducing utilization of acute care centers, administrative burdens and cost, reduced specialist utilization, and better preventive service delivery; there would be additional savings that would accrue to other government programs and self-insured employers.
The current insurance companies would be responsible for catastrophic events and specialist coverage upon referral from primary care.
How are the primary care centers paid?
Similar to the UK’s NHS, practices would be paid a per assigned member per month payment as a baseline for operations and a small profit margin. This would account for about 75% of the necessary operating costs. The remaining 25% would be paid based on performance across process and outcome measures in a manner similar to the existing Medicare Shared Savings Program, or other Accountable Care Organization models, with an incentive for primary care centers to prevent ED visits and hospitalizations. This would also remove the need for complex billing systems and staff managing payor relationships. Similarly, there could be direct payments to clinics to adopt new technologies, to incentivize the delivery of high value services, and to fund programs unique to a particular area.
There would be competition in certain areas to attract patients in order to grow revenue, thus clinics would be able to compete on quality and experience. A central health outcomes reporting system would allow all Americans to compare the care quality between clinics similar to CMS Care Compare.
How would primary care clinics operate?
Primary care clinics would offer many of the services they offer today, but a universal primary care system could allow for innovation and implementation of existing best practices at a large scale. First, an integrated center model that combines co-located behavioral health services (e.g., collaborative care), team-based care models leveraging registered nurses and dieticians for disease management, education, and care coordination, and integrated pharmacy services would allow for a one-stop shop for patients and encourage a reduction in pharmacy costs from group purchasing at the state trust level. Programs could incorporate transportation interventions and medically-tailored meals. They could have home visit programs and frequent telemedicine check-ins for high-risk patients. The health outcomes performance payment incentives would encourage clinics to adopt effective technologies, predictive analytics, and other tools to meet performance benchmarks.
Weighing the Pros and Cons
This would be a significant change, but it may be beneficial to all parties assuming one thing: that it produces better health and it results in cost avoidance. The evidence supports this hypothesis, but the devil will be in the details.
Each party receives a few key benefits:
For Patients
Guaranteed access to primary care
Access to essential medical services even during periods of unemployment
Better health
Lower expected out-of-pocket costs
The only detriment is likely the 0.25% payroll tax. But, for the vast majority of Americans this system would likely result in significant cost savings that outweigh the tax amount.
For Society
A healthier population
Better economic productivity and fewer work absence days
Reduced per capita health costs
For Primary Care Centers
Increased spending could be used for higher wages for PCPs and staff
Removal of administrative burdens from multiple payors
More interdisciplinary resources and team-based care
Continued business incentives for practice owners
For Employers
Potentially reduced costs of care for self-insured employers
Healthier and more productive workforce
For Insurance Companies
Refocus on low-frequency, catastrophic services
Potentially better profitability
There is a potential that insurance companies make fewer absolute dollars, but may be able to improve profitability due to a return to a true risk pool model.
For the Federal Government
Medicare and Medicaid may see significant continued cost savings in a few areas:
Reduced hospitalizations and ED visits
Reduced fraud, waste, and abuse7
Reduced long-term costs in Medicare due to a healthier population
Why should we expect this to work?
There are some areas of cost that are unavoidable. However, there is evidence that many ED visits and hospitalizations are entirely avoidable. It is also well understood that many procedures and specialist visits are unnecessary. By building a strong primary care system with aggressive levels of funding for evidence-based care models and interventions, both short term cost avoidance and long-term gains in health may be possible. The following bullets provide some evidence to suggest that the discussed model might be effective:
Increasing insurance coverage for the uninsured can reduce ED visits and hospitalizations
Primary care interventions have shown the ability to reduce utilization among high-users of care
Increasing funding for federally-qualified health centers has been associated with reductions in non-emergency ED visits
The challenges facing the American health care system are complex, but they're not insurmountable. A universal primary care system represents a practical, political compromise that could significantly improve health care access and outcomes while maintaining elements of the current system. This is by no means a comprehensive outline for how to accomplish this type of system redesign. There are many nuances and challenges that this approach would have to solve, but they are all surmountable.
It is important to note that while price transparency is a worthwhile goal, if the free-market proponents want to solve the problem they must deal with market consolidation among insurers and hospitals and that is often not a part of the conversation. The FTC would need the authority and resources to aggressively break up hospital systems and insurance companies both for- and not-for-profit alike. This would take decades to accomplish as these cases play out in court. Price transparency action without breaking up monopolies and oligopolies does not help.
Reproduced from the Peterson-KFF Health System Tracker at https://www.kff.org/health-policy-101-health-care-costs-and-affordability/?entry=table-of-contents-what-factors-contribute-to-u-s-health-care-spending.
Public health professionals correctly claim that health status is a multifactorial outcome that is affected by more than just the services rendered through the medical care system. Here is a good resource.
Friedberg MW, Hussey PS, Schneider EC. Primary care: a critical review of the evidence on quality and costs of health care. Health Affairs (Project Hope). 2010 May;29(5):766-772. DOI: 10.1377/hlthaff.2010.0025. PMID: 20439859.
David Blumenthal et al., Mirror, Mirror 2024: A Portrait of the Failing U.S. Health System — Comparing Performance in 10 Nations (Commonwealth Fund, Sept. 2024). https://doi.org/10.26099/ta0g-zp66
This could be done on a progressive scale if desired.
E/M code upcoding and fraud, the primary codes billed by primary care, may go down by moving to an entirely capitated payment model.